Over the past two years, a number of personnel stationed at the US embassy in Havana, Cuba, reported hearing mysterious sounds and suffering physical symptoms consistent with brain injury. At first, officials suspected that unknown sonic weapon was the cause, but that idea has faded from favor and a new theory has emerged. The new explanation? Microwaves.
Crazy as it seems, microwaves (the waves, not the ovens) can cause severe auditory symptoms. The strange auditory impacts of microwaves were first described by Allan H. Frey and Elaine Coren. In 1961, Frey and Coren noted that pulsed microwaves directed at a human or animal often created the sensations of unpleasant noises. No soundwaves are produced. The sound exists exclusively inside a person’s head and nobody else can hear it, which is consistent with reports out of Cuba that some people heard the sound while others did not.
The phenomenon is now referred to as the Frey effect, and Frey and colleagues spent decades trying to figure out exactly how it works. Writing in Science in 1979, Frey and Coren examined existing research suggesting that heat from the microwaves is the underlying cause. According to existing theories, slight elevation of the temperature in the bone and soft tissue of the head causes those tissues to expand. The expansion causes acoustic waves to form, which travel through bone to the ear where it is registered as an external sound. Frey and Coren reject portions of that hypothesis, suggesting that the thermoelastic expansion occurs directly in the cochlea of the ear, not in the head.
Government CoverUp: Havana Syndrome
How a Microwave Weapon Might Work
Personnel at the US embassy in Havana have reported mysterious sounds and physical symptoms consistent with brain injury. Could it be microwaves? By: James MacDonald, September 19, 2018
https://daily.jstor.org/how-a-microwave-weapon-might-work/
Microwave Effects on the Human Body
Introduction: Swanson et al. (1) examined 24 US Cuban embassy personnel exposed to an unknown directed energy source. They found that 21 of those examined had clinical findings similar to mild traumatic brain injury (mTBI). All 24 individuals reported audible and sometimes painful sounds during possible exposures. Hoffer et al. (2) examined a partially overlapping group of 35 embassy-related individuals, among whom 25 reported auditory phenomena and post incident symptoms along with 10 individuals who lived with the affected persons who did not report hearing sounds. These workers found that all 25 individuals hearing sounds had vestibular abnormalities; over half of these exhibited cognitive disorders. The ten individuals who did not report hearing sounds did not exhibit vestibular or cognitive abnormalities. Verma et al. (3) expanded Swanson's 2018 report to include 40 government employees describing acoustic experiences. These individuals had neurological symptoms suggesting mTBI. Significant brain structural abnormalities were documented using advanced specialized MRI imaging of this cohort (3).
The method of delivery of damaging energy to these personnel remains controversial. A sonic source initially was postulated because subjects heard high-pitched sounds during the incidents (4–8). Lin (6, 7) suggested the mode of attack as a possible directed energy source of pulsed microwaves based on observations that pulsed microwaves are audible to those irradiated. Microwaves can also be focused into narrow field-of-view beams in order to target individuals.
Experimental evidence indicates that pulsed microwaves can induce disruption in brain tissue producing subsequent behavioral and cognitive dysfunction. Thomas et al. (9) early reported that pulsed microwaves disrupted acquisition performance in rats. Wang and Lai (10) later demonstrated that acute exposures to pulsed microwaves impaired reference memory in rats. In addition, pulsed microwaves reportedly may alter blood-brain barrier permeability, disrupt long-term potentiation and result in DNA strand breaks (11). Pakhomov and Murphy (12) reviewed an extensive body of microwave experiments performed in Russia and the former Union of Soviet Socialist Republics. In these works, animal brains were found to be considerably more sensitive to pulsed microwaves than to continuous wave microwaves; they concluded that microwave heating did not, at least primarily, cause this injury effect. Thermal sensors placed in rabbit brains showed no more than a 0.2°C temperature increase in animals displaying cognitive impairments.
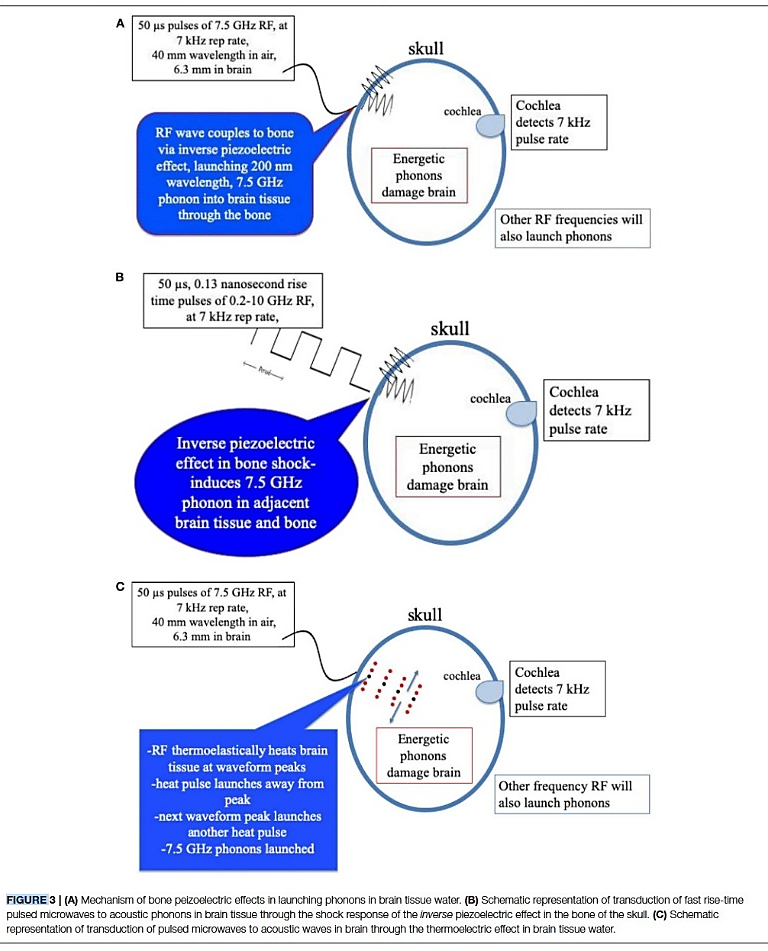
Mechanisms by which pulsed microwave energy injure or impair the brain remain unclear. Based upon our prior physical considerations of low intensity primary blast and crystalline fracture effects (13, 14), we here describe physical mechanisms by which microwave energy may produce brain injuries similar to those caused by primary blast exposure. Using documented experimental physical findings, we consider the hypothesis that primary blast shock waves due to explosions and pulsed microwaves may both excite GHz frequency phonons in brain water content to cause nanoscale subcellular brain injuries.
Pulsed Microwave Energy Transduction, Acoustic Phonon Related Brain Injury, Hubler GK., Hoffman SW., Andreadis TD. and DePalma RG. (2020) Front. Neurol. 11:753. doi: 10.3389/fneur.2020.00753; https://www.frontiersin.org/journals/neurology/articles/10.3389/fneur.2020.00753/full

The Mystery of Havana Syndrome
Gordon Corera investigates the mysterious illness that has struck American diplomats and spies. It began after some reported hearing strange sounds in Havana 2016, but reports have since spread around the world. Doctors, scientists, intelligence agents and government officials have all been trying to find out what exactly causes these sounds and the lingering health effects. Some call it an act of war, others wonder if it is some new and secret form of surveillance while others believe it could even be in the mind. So who or what is responsible?
Producer, Emma Wells, Editor, Bridget Harney.
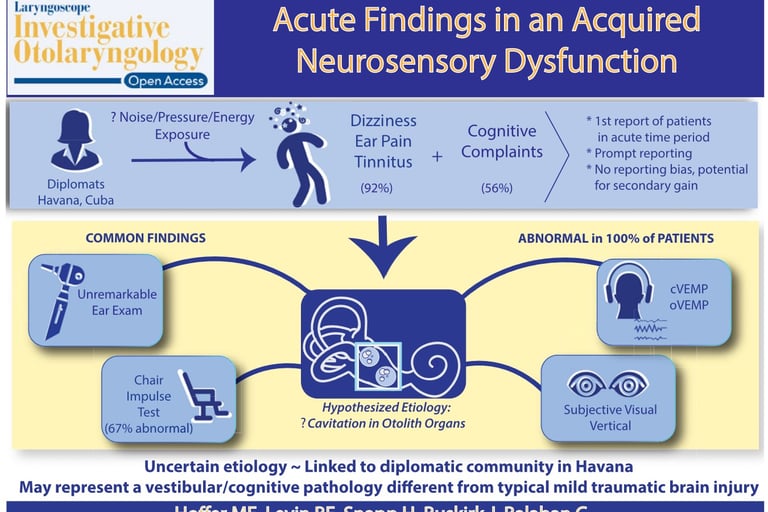
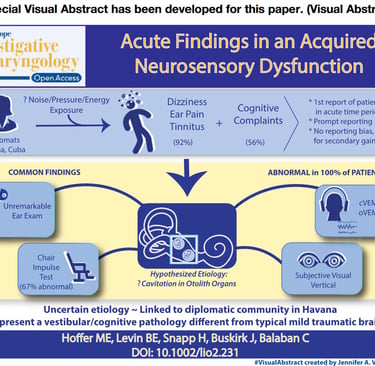
Acute Findings in an Acquired Neurosensory Dysfunction by Michael E. Hoffer, MD; Bonnie E. Levin, PhD; Hillary Snapp, AuD, PhD; James Buskirk, PT, SCS; Carey Balaban, PhD, Laryngoscope Investigative Otolaryngology published by Wiley Periodicals, Inc. on behalf of The Triological Society; https://pmc.ncbi.nlm.nih.gov/articles/PMC6383299/
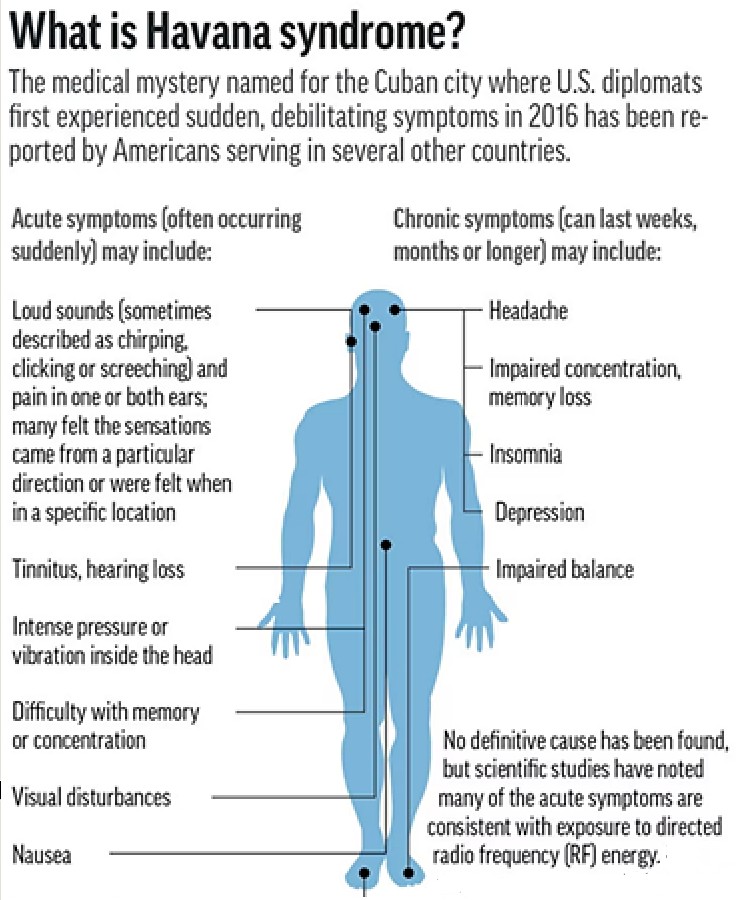
Background: In the Autumn of 2016, diplomatic personnel residing in Havana began to present with symptoms of dizziness, ear pain, and tinnitus that emerged after perception of high frequency noise and/or a pressure sensation. Understanding the acute symptoms of this disorder is important for better defining the disorder and developing optimal diagnostic, preventive, and treatment algorithms.
White papers acknowledging Havana Syndrome
are written by objective scientific community:
Objectives: To define the presenting symptoms in a cohort of patients in the acute time period after perceiving a noise/pressure exposure in Havana.
Design/Settings/Participants: Review of 25 symptomatic individuals who reported a localized sensation of noise/pressure and 10 asymptomatic individuals (roommates of those affected) who did not experience the sound/pressure.
Results: Immediately after the exposure, the majority of individuals reported intense ear pain in one or both ears and
experienced tinnitus. All of the individuals noticed unsteadiness and features of cognitive impairment. On presentation to our
center, dizziness (92%) and cognitive complaints (56%) were the most common symptoms. Formal testing revealed that 100% of individuals had an otolithic abnormality and evidence of cognitive dysfunction.
Conclusion and Relevance: This study focuses on the acute presentation of a phenomenon in which symptoms emerge after perception of a localized noise/pressure and in which the acute symptomology includes the universal nature of vestibular injuries and select cognitive deficits. The findings presented in this acute group of patients begin to provide a better picture of the initial injury pattern seen after this exposure and may allow for more accurate diagnosis of this disorder in future cases.
Key Words: Vestibular disorder, Cuba exposure, cognitive disorder, brain injury.
EXCLUSIVE: Doctors Reveal Details of Neuro-Weapon Attacks in Havana, 9/6/2018, By Stew Magnuson
Directed energy weapons intended to disrupt or damage their victims’ brains were the most likely source of a series of mysterious attacks singling out U.S. personnel assigned to the U.S. Embassy in Cuba in 2017, three doctors involved in the investigation have told National Defense in exclusive interviews.
The three experts were contacted by the State Department to investigate 25 cases of government employees working in Cuba who complained of suddenly hearing noises, pressure in their ears, followed by symptoms such as headaches, vertigo, dizziness and loss of cognitive functions.


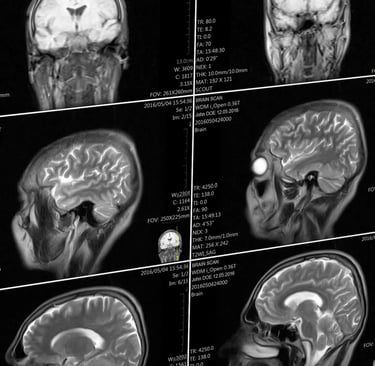
People with “Havana syndrome” have differences in their brains compared to healthy people, Nicole Wetsman, Published Popular Science Jul 23, 2019 7:00 PM EDT, https://www.popsci.com/havana-syndrome-brain-changes-mri/
"The analysis found that the patients who had been stationed in Cuba had less volume of white matter, which contains the parts of neurons that connect brain regions together, than the control groups. They had differences in their cerebellum to the control groups, and had lower connectivity in the auditory and visual networks of the brain (though not those involved in executive function).
Notably, Verma says, the patterns of changes in brain volume and in the cerebellum, were unlike the patterns of changes seen in any other diseases—they didn’t look like the changes seen in patients with traumatic brain injuries, for example, or other neurological conditions. “To the best of my knowledge, this is something unique to these patients,” she says. Seeing a new pattern, she says, is extremely rare.
The findings do indicate, though, that there are structural and functional changes in the brain that offer a potential basis for clinical symptoms. It’s a counter to some criticisms levied on the team’s prior paper that evaluated the neurological symptoms of this patient group, which included skepticism that their experiences weren’t just psychogenic. “The clinical element said there should be a problem in the cerebellum, and the imaging showed changes in the cerebellum. It’s an objective measure,” Verma says.
However, it’s not clear what the overall changes seen in this study mean clinically, for patient function, according to an accompanying editor’s note also published in the JAMA. It’s also not clear how significant the changes between the two groups are, says Gerard Gianoli, a neurotologist (someone who specializes in neurological disorders of the ear) at the Ear and Balance Institute in Louisiana. Gianoli says he’s more convinced by a 2018 paper that showed inner ear damage in those affected. The new paper, though, still provides important data. “It’s a part of the puzzle, and it adds a piece of information,” he says.
The changes in these patients, both in the brain and in the inner ear, could be caused by multiple different things, Gianoli says—this research doesn’t answer questions about the initial trigger. It may never be clear what happened, Verma says. “If you asked me, did something happen, I would say yes. But this doesn’t tell us how or why.” Americans reported hearing torturous sounds in Cuba—and now their brains seem changed.

Bartholomew RE, Baloh RW. "Havana Syndrome": A post mortem. Int J Soc Psychiatry. 2024 Mar;70(2):402-405. doi: 10.1177/00207640231208374. Epub 2023 Dec 25. PMID: 38146090; PMCID: PMC10913303; University of Auckland, Building 503, 85 Park Road, Auckland 1023, New Zealand;
https://pmc.ncbi.nlm.nih.gov/articles/PMC10913303/
Excerpt:https://www.goodreads.com/book/show/52576972-havana-syndrome
"The withholding of information. While the U.S. Government allowed the release of the NAS findings, they withheld the results of other investigations that were skeptical of the condition. In 2018, the Federal Bureau of Investigation concluded that mass psychogenic illness was most likely responsible for the outbreak. While the report remains classified, its conclusions were leaked to the media. The contents of a second classified report were only released in September 2021 after a Freedom of Information Act filing. It found the role of microwave radiation “highly unlikely,” and that psychogenic illness appeared to play a role (Declassified U.S. Government Study, 2018, p. 8). The authors obtained and analysed several recordings of mysterious sounds that victims said coincided with their symptoms. They were identified as the mating call of the Indies short-tailed cricket. This was significant because victims had been counseled to be hypeaware of unusual sounds that were presumably from a foreign adversary. The report also noted that, contrary to the NAS findings, the sounds could not have been evidence of microwave radiation as such waves cannot be captured on an audio recording. The NAS panel was unaware of these findings as the report had not been shared.
Hiding in Plain Sight Havana Syndrome is a case of old wine in new skins. Despite its novel appearance, it embodies key elements of two longstanding moral panics. The first is the “enemy at the gate”—the fear of an imminent threat from nefarious foreigners intent on causing harm to one’s country or its citizens. Common xenophobic scapegoats in American history include the fear of Chinese, Russians, Japanese, Jews, and Muslims. The second fear involves health threats from new technologies which can be traced back centuries from the belief that listening to the strains of certain musical instruments could cause illness to concern that exposure to electric lights would induce blindness (Baloh & Bartholomew, 2020). Contemporary examples include health worries involving mobile phones, Wi-Fi, 5G, and wind turbines. “Havana Syndrome” is just the latest in a long list of health scares. In October 2021, the U.S. Congress passed a law authorizing financial compensation for government victims of “Havana Syndrome.” This is reminiscent of past decisions to award compensation for dubious conditions such as “railway spine” in the U.K. (Gasquoine, 2020) and “telephone sickness” in German switchboard operators (Killen, 2003). Over the course of their 6-year investigation into “Havana Syndrome” U.S. officials expended considerable human capital and financial resources going down a rabbit hole searching for exotic explanations. Instead of finding secret weapons and foreign conspiracies—they found only rabbits. For in the end, prosaic explanations were determined to be the cause of the events in Cuba and its subsequent global spread. That is the lesson of “Havana Syndrome”—follow the science."
White papers denying Havana Syndrome written by government agencies:
NIH studies find severe symptoms of “Havana Syndrome,” but no evidence of MRI-detectable brain injury or biological abnormalities, Monday, March 18, 2024, National Institutes of Health (NIH)-https://www.nih.gov/news-events/news-releases/nih-studies-find-severe-symptoms-havana-syndrome-no-evidence-mri-detectable-brain-injury-or-biological-abnormalities
"Using advanced imaging techniques and in-depth clinical assessments, a research team at the National Institutes of Health (NIH) found no significant evidence of MRI-detectable brain injury, nor differences in most clinical measures compared to controls, among a group of federal employees who experienced anomalous health incidents (AHIs). These incidents, including hearing noise and experiencing head pressure followed by headache, dizziness, cognitive dysfunction and other symptoms, have been described in the news media as “Havana Syndrome” since U.S. government personnel stationed in Havana first reported the incidents...“It is possible that individuals with an AHI may be experiencing the results of an event that led to their symptoms, but the injury did not produce the long-term neuroimaging changes that are typically observed after severe trauma or stroke. We hope these results will alleviate concerns about AHI being associated with severe neurodegenerative changes in the brain.”
"...our analysis indicates several of the 'victims' in these cases may have experienced an episode of Mass Psychogenic Illness or social contagion." FBI heavily redacted study, March 18, 2019; https://static01.nyt.com/newsgraphics/documenttools/8f51fc1ea6ff1dce/fe01a257-full.pdf
A senior Defense Department official who attended last year’s NATO summit in Vilnius, Lithuania, [July 12, 2023] had symptoms similar to those reported by U.S. officials who have experienced “Havana syndrome,” the Pentagon confirmed Monday. Havana syndrome is still under investigation but includes a string of health problems dating back to 2016, when officials working at the U.S. Embassy in Havana reported sudden unexplained head pressure, head or ear pain, or dizziness. US defense official had ‘Havana syndrome’ symptoms during a 2023 NATO summit, the Pentagon confirms. By TARA COPP, Updated 5:40 PM EST, April 1, 2024; https://apnews.com/article/havana-syndrome-russia-cuba-vilnius-4839ec0e3ce0db76670832235d602a16
The rapid advancement of neuroscience and its corresponding technologies has prompted renewed and growing interest in both its development and the ethical concerns about the use of such techniques and tools in military and security contexts.
In 2008, the National Research Council of the National Academies of Science reported that the brain sciences showed potential for military and warfare applications, but were not yet wholly viable for operational use. However, by 2014, a subsequent report of the National Academies, “Emerging and Readily Available Technologies and National Security: A Framework for Addressing Ethical, Legal and Societal Issues,” concurred with a series of white papers by the strategic multilayer assessment group of the Joint Chiefs of Staff, and a 2013 Nuffield Council Report, stating that developments in the field had progressed to the extent that rendered the brain sciences viable, of definitive value and a realistic concern for the military.
This timeline is important, as it reflects the rapid and iteratively more sophisticated capability to create and exploit neuroscientific methods and technologies to access the brain, and assess and affect its functions of cognition, emotion and behavior.
Advancements in neuroscience could be used to create “super soldiers,” link brains to weapon systems for command and control, or even manipulate groups or leaders into taking actions that they normally wouldn’t do.
Obviously, new developments in brain science can be harnessed to improve neurological and psychiatric care within military medicine, and a number of ongoing Defense Department programs are doing so. The Defense Advanced Research Projects Agency, the Army Medical Research and Materiel Command and the Naval Bureau of Medicine and Surgery are generating new techniques and technologies for treating brain injury, neurodegenerative diseases such as Parkinson’s and Alzheimer’s disease, and certain psychiatric conditions, such as post-traumatic stress disorder and depression.
However, there is also considerable potential for dual-use applications of neuroscientific methods and tools that extend beyond the bedside. Many of these may reach battlefields.
These include the use of various drugs and forms of neurotechnologies such as neurofeedback, transcranial electrical and magnetic stimulation, and perhaps even implantable devices for training and performance optimization of intelligence and combat personnel. Brain-computer interfaces could be used to control aircraft, boats or unmanned vehicles. Military and warfare uses also entail the development and engagement of agents — such as drugs, microbes, toxins — and “devices as weapons,” also called neuroweapons, to affect the nervous system and modify opponents’ thoughts, feelings, senses, actions, health or — in some cases — to incur lethal consequences.
The use of neuroscience and technology to optimize the performance of military personnel could potentially lead to the creation of “super soldiers.” This remains a provocative and contentious issue.
When viewed in a positive light, such approaches could — and arguably should — be employed to prevent warfare. For example, intelligence and military personnel who have increased cognitive, emotional and/or behavioral capacities might be able to more easily and capably detect threats, function under arduous conditions with less stress, and have increased sensitivity to socio-cultural and physical cues and nuances in foreign environments. They could be more effective in reducing the risk of violence.
These goals led to efforts such as the Intelligence Advanced Research Projects Activity’s Sociocultural Content in Language program and the Metaphor program, which both sought to improve insight into cultural linguistic and emotional norms. DARPA’s Narrative Networks program aimed to utilize neurocognitive science and technology to improve narratives in socio-cultural contexts.
On the other hand, there are concerns for the negative effects that the field might have on “neuro-modified” individuals’ health. There is trepidation about using such approaches to turn warfighters into amoral, combative automatons and questions about what responsibilities and burdens might be incurred for — and borne by — the military, and perhaps society at large, when dealing with such effects.
But while such questions and concerns may suggest the need for a reflective pause, it’s important to note that brain research and its corresponding technologies are becoming ever more international, and a number of countries such as China and Russia, and some U.S. allies, are engaged in these pursuits and are interested in their military viability and use. This creates a situation that tends to sustain, if not advance the pace and extent of research, development and incorporation of neuroscience and technology in intelligence and military initiatives.
The internationalization of brain science, taken together with the speed of its progress, fosters additional concerns about the development and use of neuroweapons.
While existing international agreements on biological and chemical weapons such as the Hague Conventions, Geneva Protocol and the Biologic, Toxin and Weapons Convention limit institutional research, stockpiling and international trade of certain toxins and neuro-microbiologicals such as ricin and anthrax, some neurobiological substances and technologies developed for medical products that are readily available on the commercial market might not fall within existing international rules.
These include neurotropic drugs created in pharmaceutical labs, bio-regulators — defined as substances that affect biological processes, such as opioids and other peptides — and neuromodulatory technologies such as transcranial or deep brain stimulating devices.
And, as noted in the 2008 National Academy of Sciences report, products intended for the health market can — and frequently are — studied and developed for possible employment in military applications. In the United States, any such activity in federally funded programs would be subject to oversight in accordance with dual-use policies, reflecting the general tenor of current international biological and chemical weapons conventions.
The increasing availability of tools for DIY neurobiology, such as gene-editing kits that can be employed to genetically modify existing microbes and toxins and make them more potent or lethal, increases the probability of both their use, and attendant risks and threats that such techniques and their products pose to national security. Former Director of National Intelligence James Clapper stated last year that gene editing should be regarded for its potential for creating biological weapons. [Morgellons has already been put in many Targeted Individuals]
The impact of neuroweapons is equally important to consider. While nerve agents such as sarin, or pathogens such as anthrax, can induce somewhat widespread effects, other, more sophisticated neuroweapons should not be regarded as weapons of mass destruction, but rather as “weapons of mass disruption,” often with subtle, albeit intensifying effects.
For instance, neurologically acting drugs can be used to selectively target the thoughts, sentiments and actions of an individual, such as a political or military leader, to evoke a change in his or her ideas, emotions and behavior. This could exert effect on those they lead, influencing their views and actions toward either conformity or dissonance.
Certain neuroactive drugs, toxins and/or microbes can also be used against larger scale targets to incur “ripple consequences” within a group, community or population. For example, these agents could be dispersed to produce “sentinel cases” of individuals who exhibit neuro-psychiatric and other physical signs and symptoms. Attribution as a terrorist action, and accompanying misinformation about salient and escalating signs and symptoms — such as anxiety, sleeplessness and paranoia — could be propagated over the internet.
Brain science confers powerful capabilities to affect “minds and hearts” and therefore affords clear and present leverage in military and warfare operations.
Join us in advocating against harmful technology misuse.
contact@targetedhumans.org
© 2025. All rights reserved.
Targeted Humans Inc.